

National Survey on Lupus Report: Part One

Report highlights
- Medication treatment
- Access to healthcare services
- Daily and physical activity limitations
- Impact on employment
- Quality of life
- Accessing Information, education and support
- How can survey findings guide us
Lupus is a complex autoimmune disease that affects nearly every part of life, including health, work, family and emotional wellbeing. Lupus’ unknown potential causes are thought to range from a person’s genetics to environmental factors, such as sunlight or certain types of infection, that can make the diagnosis and management of lupus challenging. Even though we’ve seen advancements in treatment, many people in Canada living with lupus continue to face barriers to timely and appropriate health care and support.
To better understand the lived experience of people with lupus, Arthritis Consumer Experts conducted a national English and French online survey from September 16, 2025, to October 30, 2025, with a focus on:
- diagnosis and treatment journey
- access to care and medications
- activity limitations
- impact on work and daily life
- patient support needs
The online survey was co-developed by patient representatives from ACE and Lupus Canada and experts from the Lupus Working Group, including researchers, academia, and health care professionals. This JointHealth™ insight report shares findings and what we heard in respondents’ comments and highlights the changes needed to improve lupus care in Canada.
What is lupus?
Lupus is the common name for a family of autoimmune diseases where the immune system mistakenly attacks healthy tissues. It can affect the skin, joints, kidneys, lungs, heart, blood cells, and brain. Symptoms often come and go, making diagnosis difficult. They can also mimic other diseases or behave differently amongst those affected. The most common type of lupus is Systemic Lupus Erythematosus (SLE). Lupus affects approximately 1 in 1000 Canadians. Anyone can get lupus. But certain people are at higher risk for lupus, including:
People who have a family member with lupus or another autoimmune disease
- Women ages 15 to 44
- Certain racial or ethnic groups, including people who are Indigenous, Black, or People of Colour.1,2
- People who have a family member with lupus or another autoimmune disease
Who responded to the Survey?
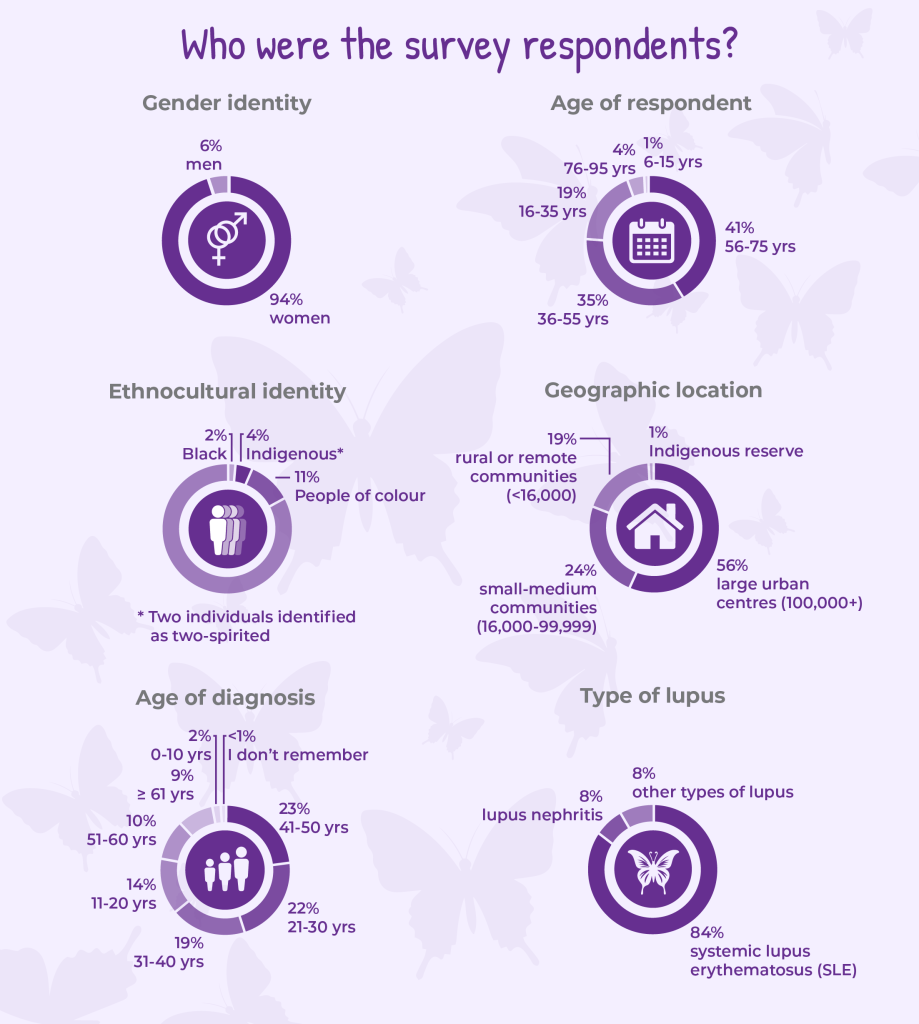
There was a total of 248 respondents – 213 of whom had been diagnosed with lupus by a health care professional and were prompted to continue the Survey.
Most survey respondents were diagnosed between the ages of 21 and 50 and 94% were women, reflecting the reality that lupus most often strikes people during their prime working and child-bearing years and disproportionately affects women. In Canada and globally, about 9 out of 10 people living with lupus are women.3
Research studies show that lupus is much more common in Black, Indigenous, Hispanic/Latina, and Asian populations in Canada and when they develop it, it is more severe disease and results in worse outcomes compared with white populations.4
In our survey, only 4 percent of respondents identified as Indigenous and 13 percent as Black or other people of colour combined, which is a limitation when considering the results of our crowd sourced survey.
Key findings
Diagnosis pathway
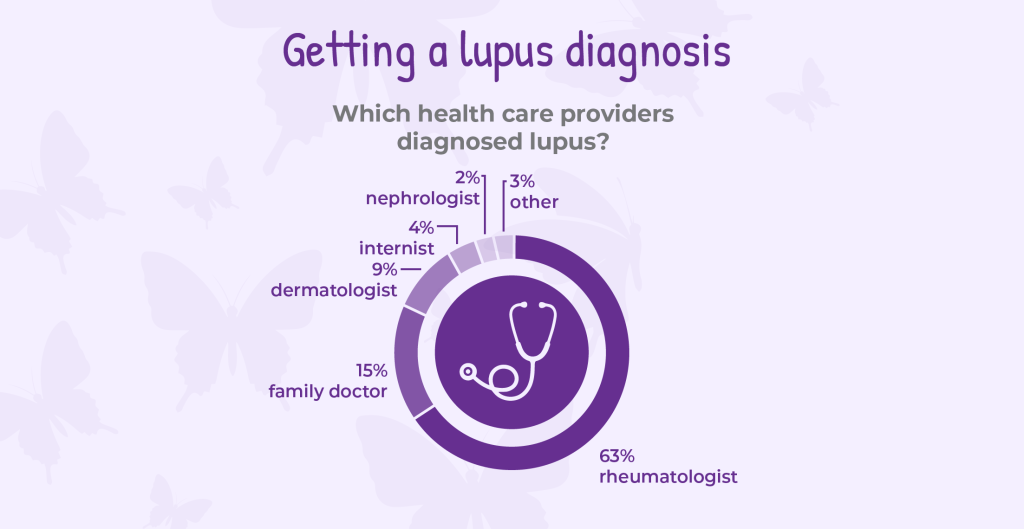
Nearly two-thirds of our respondents were diagnosed by a rheumatologist, while others received diagnoses from dermatologists, internists, and nephrologists. However, respondents said getting a diagnosis for lupus was challenging. For many, it came only after misdiagnosis, having their symptoms ignored or dismissed, or difficulty accessing a specialist.
Which health care providers diagnosed lupus?
- 63% were diagnosed by a rheumatologist
- 15% by a family doctor
- 9% by a dermatologist
- 4% by an internist
- 2% by a nephrologist
- 3% other (pediatrics, chiropractor, nurse practitioner)
What respondents told us
“Dismissed, ignored, misdiagnosed, told it’s in my head, told I dwell on health too much, not believed, I was even accused by a rheumatologist of copying symptoms off the internet??? (I didn’t – I wrote down what I was experiencing), the rheumatologists have been horrible and a saw a horrible dermatologist that made me feel so worthless, I have had drs in ER yell at me, I been told I am too medically complicated.”
– Woman, born between 1970-1989, from a large urban center
“I believe the main issue with receiving an appropriate diagnosis and care for lupus is the difficulty of accessing a rheumatologist, as well as general practitioners’ and internists’ belief that specialists should not be bothered. This can lead to a deterioration in the patient’s health that could be avoided with faster diagnosis and care.”
– Man, born between 1950-1969, from a large urban center
Medication treatment
Respondents said they experienced challenges accessing treatment and care after their diagnosis. While 64% of respondents said they were very satisfied or satisfied with their current lupus treatment, 19% reported they were dissatisfied or very dissatisfied.
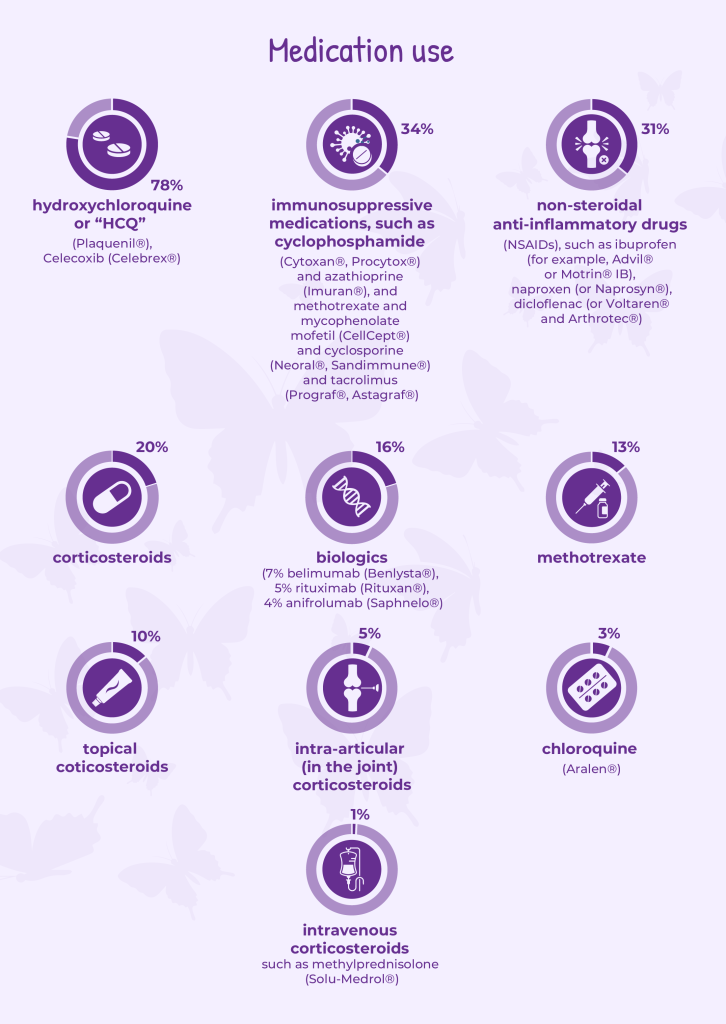
Medication use was high among survey respondents:
- Three in four reported taking hydroxychloroquine
- 36% taking corticosteroids
- 34% taking immunosuppressive medications
- 31% taking over-the-counter pain relievers
- 16% taking biologic therapies
Expert guidelines recommend access to specific lupus medicines. However, access to essential prescription medications was not equal. When asked how easy or difficult it was to receive reimbursement access to medications prescribed for their lupus:
- 57% of respondents selected either very easy or easy
- 18% selected neutral
- 12% selected difficult or very difficult
The survey results shows that financial barriers still prevent some patients from receiving optimal care, even when effective treatments exist.
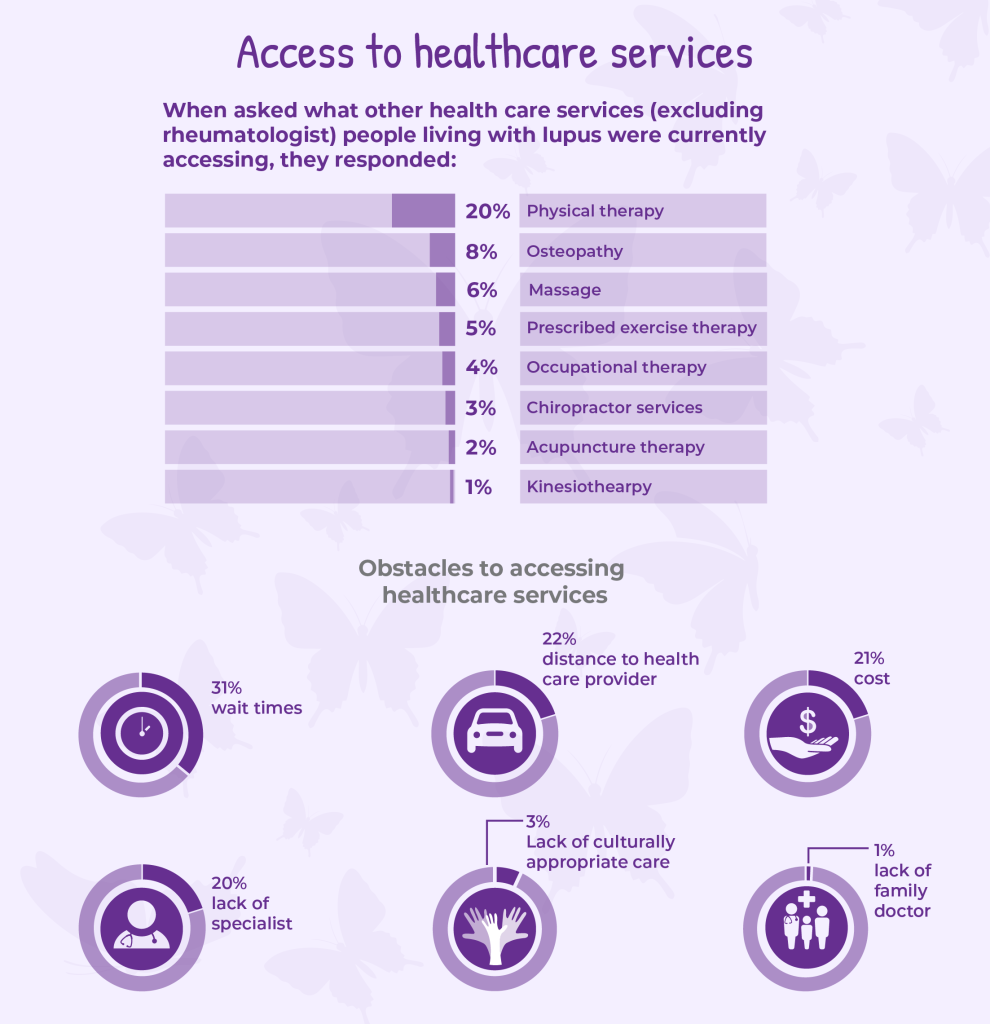
Access to healthcare services
Current lupus treatment guidelines developed by medical experts emphasize that medications alone are not enough to fully manage the disease. Both European League Against Rheumatism and American College of Rheumatology guidelines stress the importance of interprofessional healthcare services, such as physical/occupational/exercise therapy, as part of comprehensive lupus care.5,6 Yet, 62% of survey respondents reported that they were not accessing any arthritis health professional services, including physiotherapy, occupational therapy, or prescribed exercise.
Among the challenges in accessing treatment and care after their diagnosis, one in three respondents reported long wait times for care, while other respondents said that distance to providers (22%), cost (21%), and lack of access to specialists (20%) were major barriers. This suggests that treatment guidelines and real-world lupus care delivery across Canada don’t match up. Clinical standards recommend timely access to healthcare services, but many people in Canada with lupus cannot access that care when they need it.
These access challenges are especially concerning for Indigenous, Black, and People of Colour. Research consistently shows that racialized patients are more likely to experience diagnostic delays and disease complications. When structural barriers such as geography, cost, and system navigation are layered on top of these risks, inequities deepen further.
What respondents told us
“My rheumatologist is 45 minutes away. I drive from a rural town into Brampton. I don’t drive in the city. The parking lot is paid. The pay machine is very slow and not sheltered from the sun. The elevators are usually out and I have to climb 3 flights of stairs. My appointments are no more than 10 minutes long. Where are the physical checkups?”
– Woman, born between 1970-1989, from a rural or remote community
“Difficulty finding knowledgeable doctors who will treat the whole body.”
– Woman, born between 1950-1969, from a small-medium sized population centre
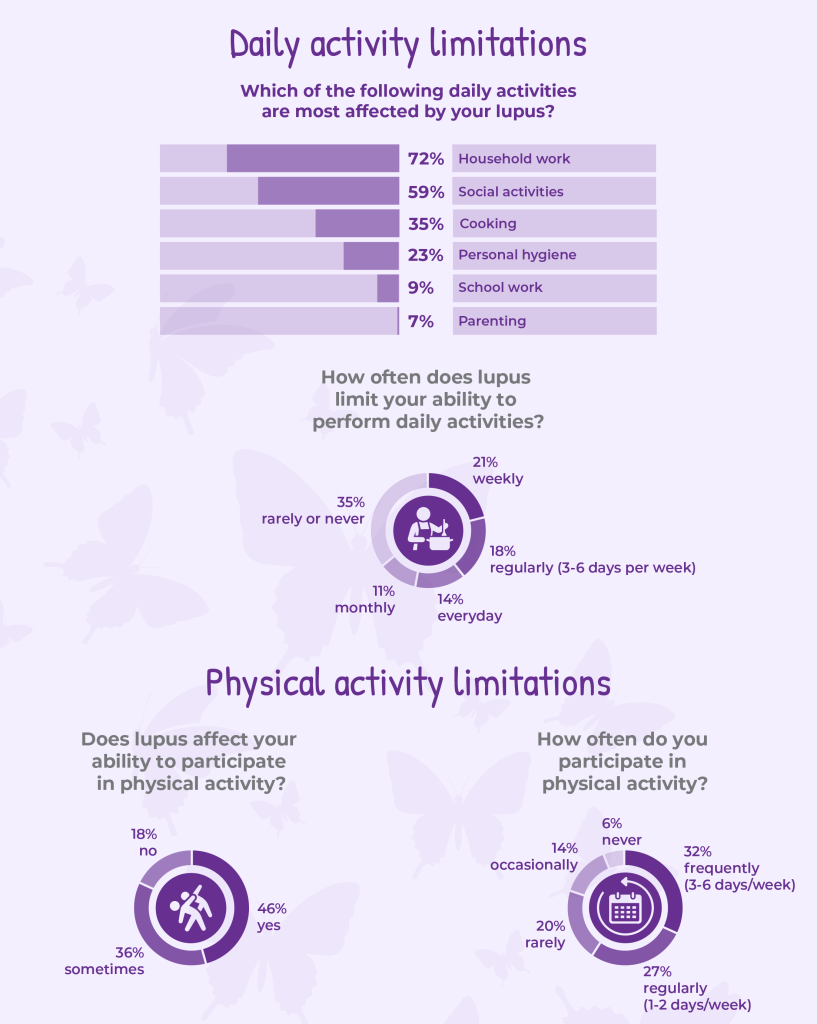
Daily/physical activity limitations
The survey findings show that lupus has a persistent and meaningful impact on day-to-day functioning and physical activity for many respondents. A majority reported regular limitations in daily activities, most often affecting household work (72%) and social activities (59%). Nearly one in three respondents said lupus limits their daily activities weekly or more often, and another one in seven experience limitations every day. Together, these findings point to a sustained level of functional impairment that shapes how people live, work, and engage with others.
Physical activity is similarly affected. Physical activity includes recreational activities, individual exercise, team sports, exercise programs or classes, cardiovascular training, strength-based training, and household work like gardening and vacuuming.
While regular movement is widely recommended as part of lupus care7, 46% of respondents said lupus affects their ability to participate in physical activity, and another 36% said it sometimes does. Only a small minority reported being able to exercise without limitation. Although some respondents were able to engage in physical activity regularly, many described doing so infrequently or not at all, reflecting the ongoing challenges of fatigue, pain, and unpredictable flares.
What respondents told us
“Parenting: but mostly the kid’s activities. I missed out on seeing them play a sport, etc. Personal hygiene: there are days where I wait to take a shower until someone is home. I am not always steady on my feet. And honestly, taking a shower is EXHAUSTING. you shouldn’t need to lie down after washing your hair. But I do most days.”
– Woman, born between 1950-1969, from a large urban center
“Has put me behind in school as I’ve had to miss lectures and end up falling behind. Professors are not understanding.”
– Woman, between 1990-2009, from a small-medium sized population centre
“I’m tired but I keep going, including walking outdoors daily for an hour (rain or shine). The first 15mins is hard because my body doesn’t feel like moving but if I keep going, the fatigue and stiffness/pain go away and I feel good after. I sleep an average of 8hrs/night. I eat a balanced diet and avoid alcohol (except on holidays/family gathering). I also pray everyday and go to church every Sunday.”
– Woman, born between 1970-1989, from a rural or remote community e
Significant impact on employment
In terms of how lupus impacted their work experience, one in five respondents reported being unable to work due to lupus, and another one in five had reduced their working hours.*
Many rely on sick leave, unpaid leave, or disability benefits to manage their disease. It is important to note that survey respondents were generally older adults which may have influenced these findings.
These findings reflect a major gap between clinical treatment goals and real-world social outcomes. Expert guidelines focus on preserving function and participation, but the survey shows that many people with lupus experience significant work disruption and long-term income insecurity.
This economic vulnerability is particularly concerning for racialized and lower-income patients, who are more likely to work in jobs with limited security and few benefits. When lupus disrupts employment, financial strain further limits access to medications, therapies, and mental health supports.
* Please note that 12% respondents living with lupus were retired and 7% of caregivers of people living with lupus were retired. Because many survey respondents were older and no longer in the workforce, survey findings may underestimate the true impact of lupus on employment.

Respondents who selected “other” were asked to elaborate:
“I am self-employed. I can manage my own workload around my lupus. Working at home allows me to have easy access to the things I need to manage my Lupus and allows me to flexibility to rest when I need to. I would never survive being in the workforce, but having my own business allows me to work around and with my Lupus so that I can still earn an income and have purpose for my life.”
– Woman, born between 1950-1969, from a rural or remote community
As a follow up question, respondents were asked if providing care and supporting them has affected the employment of their caregiver (family member, friend, or other support person).
- 20% take sick days or unpaid leave
- 5% request workplace accommodations
- 4% reduce working hours or switch to part-time work
- 3% unable to work
- 2% leave a job or change careers
The remaining 6% of respondents selected “I do not have a caregiver”.
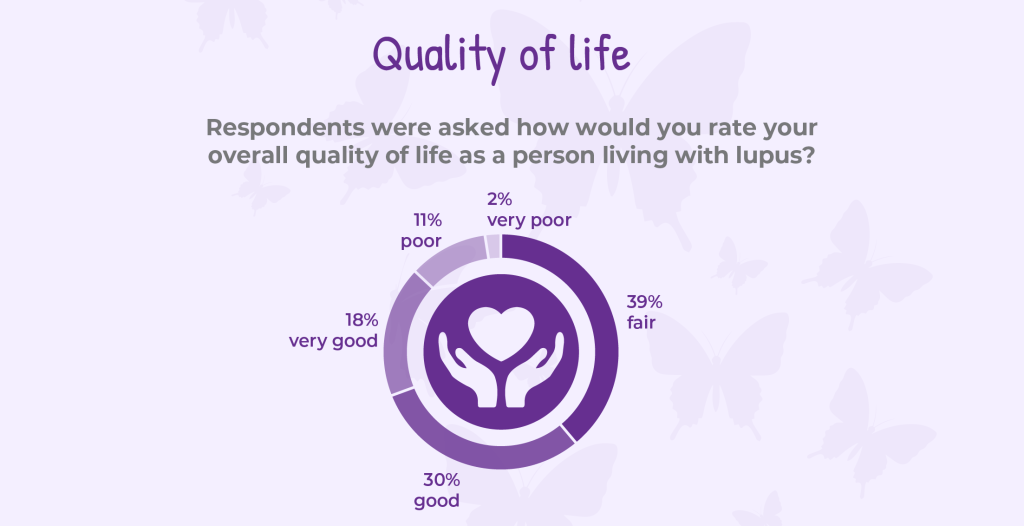
Quality of life
Living with lupus affects far more than physical health. It shapes how people feel day to day, how they plan their lives, and how much energy they have for work, family, and the activities that bring joy and meaning. When asked to rate their overall quality of life, responses revealed in open-ended comments a wide range of experiences, but also a clear signal of ongoing burden. While close to 50% of respondents described their quality of life as good or very good, just as many reported living with fair, poor, or very poor quality of life. Unpredictable symptoms, chronic fatigue, pain, and flares continue to limit daily functioning and make it difficult to work or do household chores, plan ahead, sustain social connections, or enjoy physical activities that were once routine.
Many respondents provided insightful open-ended responses:
“I was thinking of this the other day as I was sitting in the ER getting IV. I used to love the beach and going out and now sunny days make me so sick. I took my grandkids to the farm with my daughter for an event and that day at the farm has left me with months and months and months of sickness due to allergies sunshine I don’t know too much work. I have zero energy always tired, always sore. It’s hard to be happy. It’s hard to have fun but if I start crying, I fear I’ll never stop so I just usually say “meh” and just keep trucking along the best I can.”
– Woman, born between 1970-1989, from a large urban center
“It’s difficult to plan anything or having to cancel plans at last minute. You never know how you will wake up each day and what symptoms you will have to deal with. The fatigue can be debilitating.”
– Woman, born between 1950-1969, from a rural or remote community
People looking for accessible information, education, and support
Living well with lupus requires having timely, trustworthy information, practical self-management tools, and meaningful support. When asked what resources would better support their life with lupus, respondents highlighted clear gaps in education and support that affect their ability to manage symptoms, make informed decisions, and advocate for themselves. Many expressed a strong desire for up-to-date information on research advances (59%), guidance on everyday self-management strategies (45%), and access to mental health support (40%).
The findings reflect a need for education and support that is practical, accessible, and responsive to the real-world challenges of living with an unpredictable and complex disease.
When asked what resources would better support their life with lupus, respondents indicated one or more items they wanted:
- 59% information on research advances
- 45% webinars on the topic of self-management through physical activity, diet, pacing, joint protection strategies
- 40% mental health support
- 34% online education programs to learn more about my type of lupus
- 33% information on how to talk to an employer about lupus and how it impacts work life
- 28% connecting online with other people with lupus
The remaining 16% of respondents selected “other” and were asked to specify:
“The impact lupus has on female hormonal changes.”
– Woman, born between 1970-1989, from a large urban center
“More information on recovering from an injury or surgery when you have lupus, as it takes longer and other doctors don’t understand why it takes so long to recover.”
– Woman, born between 1970-1989, from a large urban center
“I am very discouraged there is no support Lupus sharing circle on my home First Nations territory. I would love to talk with others who have been stricken with Lupus. The Lupus journey for me is a lonely one. There is no Lupus help available to me where I live.”
– Woman, born between 1950-1969, resides on a First Nations, Métis, or Inuit reserve/settlement
“Information on how to advocate for one’s self when physicians don’t believe symptoms without photos – allowing easy access to pain meds when needed (without photographs of swollen joints or rashes).”
– Woman, born between 1970-1989, from a large urban center
How can lupus survey findings guide us?

Survey findings reveal substantial unmet needs among people living with lupus in Canada. Respondents described difficulty accessing specialists, inconsistent medication coverage, and significant employment and functional limitations. Respondents also identified critical gaps in education and self-management resources.
Expert guidelines also emphasize the importance of physical activity, physiotherapy, and non-medication supports to preserve function and quality of life. Yet the survey shows that many people with lupus are living with ongoing limitations while lacking access to the supports that could help them manage symptoms safely and sustainably.
These insights highlight urgent opportunities for governments to recognize lupus as a disability for benefits and workplace accommodations; for health systems and insurers to improve access to physiotherapy, safe physical activity supports, and other non-medication care that helps people maintain function and quality of life; for public and private drug plans to expand reimbursement coverage for lupus medications; and for advocacy organizations to provide more patient-centred online, education and support programs.
References
- Izmirly, P. M., Parton, H., Wang, L., McCune, W. J., Lim, S. S., Drenkard, C., Ferucci, E. D., Dall’Era, M., Gordon, C., Helmick, C. G., & Somers, E. C. (2021). Prevalence of Systemic Lupus Erythematosus in the United States: Estimates From a Meta-Analysis of the Centers for Disease Control and Prevention National Lupus Registries. Arthritis & rheumatology (Hoboken, N.J.), 73(6), 991–996. https://doi.org/10.1002/art.41632
- Fatoye, F., Gebrye, T., & Svenson, L. W. (2018). Real-world incidence and prevalence of systemic lupus erythematosus in Alberta, Canada. Rheumatology international, 38(9), 1721–1726. https://doi.org/10.1007/s00296-018-4091-4
- Pons-Estel, G. J., Alarcón, G. S., Scofield, L., Reinlib, L., & Cooper, G. S. (2010). Understanding the epidemiology and progression of systemic lupus erythematosus. Seminars in arthritis and rheumatism, 39(4), 257–268. https://doi.org/10.1016/j.semarthrit.2008.10.007
- Hurd, K., & Barnabe, C. (2017). Systematic review of rheumatic disease phenotypes and outcomes in the Indigenous populations of Canada, the USA, Australia and New Zealand. Rheumatology international, 37(4), 503–521. https://doi.org/10.1007/s00296-016-3623-z
- Parodis, I., Girard-Guyonvarc’h, C., Arnaud, L., Distler, O., Domján, A., Van den Ende, C. H. M., Fligelstone, K., Kocher, A., Larosa, M., Lau, M., Mitropoulos, A., Ndosi, M., Poole, J. L., Redmond, A., Ritschl, V., Alexanderson, H., Sjöberg, Y., von Perner, G., Uhlig, T., Varju, C., … Boström, C. (2024). EULAR recommendations for the non-pharmacological management of systemic lupus erythematosus and systemic sclerosis. Annals of the rheumatic diseases, 83(6), 720–729. https://doi.org/10.1136/ard-2023-224416
- Sammaritano, L. R., Askanase, A., Bermas, B. L., Dall’Era, M., Duarte-García, A., Hiraki, L. T., Son, M. B. F., Werth, V. P., Aranow, C., Barnado, A., Broder, A., Brunner, H. I., Chong, B. F., Chowdhary, V. R., Hersh, A. O., Izmirly, P. M., Jules, M., Kalunian, K., Kamen, D., Rubinstein, T. B., … Mustafa, R. A. (2025). 2025 American College of Rheumatology (ACR) Guideline for the Treatment of Systemic Lupus Erythematosus. Arthritis care & research, 10.1002/acr.25690. Advance online publication. https://doi.org/10.1002/acr.25690
- Blaess, J., Geneton, S., Goepfert, T., Appenzeller, S., Bordier, G., Davergne, T., Fuentes, Y., Haglo, H., Hambly, K., Kinnett-Hopkins, D., Su, K. Y., Legge, A., Li, L., Mak, A., Padjen, I., Sciascia, S., Sheikh, S. Z., Soriano-Maldonado, A., Ugarte-Gil, M. F., Md Yusof, M. Y., … Arnaud, L. (2024). Recommendations for physical activity and exercise in persons living with Systemic Lupus Erythematosus (SLE): consensus by an international task force. RMD open, 10(2), e004171. https://doi.org/10.1136/rmdopen-2024-004171
Listening to you
We hope you find this information of use. Please tell us what you think by writing to us or emailing us at feedback@jointhealth.org. Through your ongoing and active participation, ACE can make its work more relevant to all Canadians living with arthritis.
Update your email or postal address
Please let us know of any changes by contacting ACE at feedback@jointhealth.org. This will ensure that you continue to receive your free email or print copy of JointHealth™ insight.
Arthritis Consumer Experts (ACE)
Who We Are
Arthritis Consumer Experts (ACE) and its team members acknowledge that they gather and work on the traditional, ancestral and unceded territory of the Coast Salish peoples -ʷməθkʷəy̓əm (Musqueam), Sḵwx̱wú7mesh (Squamish), and Səl̓ílwətaʔ/Selilwitulh (Tsleil-Waututh) Nations.
Arthritis Consumer Experts (ACE) operates as a non-profit and provides free research based education and information to Canadians with arthritis. We help (em)power people living with all forms of arthritis to take control of their disease and to take action in healthcare and research decision making. ACE activities are guided by its members and led by people with arthritis, scientific and medical experts on the ACE Advisory Board. To learn more about ACE, visit www.jointhealth.org
Disclosures
Over the past 12 months, ACE received financial and in-kind support from: Amgen Canada, Arthritis Research Canada, Arthritis Society Canada, Biogen Canada, Canadian Biosimilars Forum, Canadian Rheumatology Association, Celltrion Healthcare Canada, JAMP Pharma, Novartis Canada, Organon Canada, Pfizer Canada, Sandoz Canada, UCB Canada, and the University of British Columbia.
ACE also received unsolicited donations from its community members (people with arthritis) across Canada.
ACE thanks funders for their support to help the nearly 6 million Canadians living with osteoarthritis, rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis and the many other forms of the disease.
Disclaimer
The material contained on this website is provided for general information only. This website should not be relied on to suggest a course of treatment for a particular individual or as a substitute for consultation with qualified health professionals who are familiar with your individual medical needs. Should you have any healthcare related questions, you should contact your physician. You should never disregard medical advice or delay in seeking it because of something you have read on this or any website.
This site may provide links to other Internet sites only for the convenience of World Wide Web users. ACE is not responsible for the availability or content of these external sites, nor does ACE endorse, warrant or guarantee the products, services or information described or offered at these other Internet sites.
Although the information presented on this website is believed to be accurate at the time it is posted, this website could include inaccuracies, typographical errors or out-of-date information. This website may be changed at any time without prior notice.